Blog
Latest News
Cardiovascular Diseases (CVD) in India
-in-India.jpeg)
Cardiovascular Diseases (CVD) in India
By Brandbugle
1. Introduction: 32% of the adult deaths in India in the time frame from 2010 to 2013 were attributed to Cardiovascular Diseases (CVD). The World Health Organisation (WHO) has also highlighted the increasing trends in Years of Life Lost (YLLs) and Disability Adjusted Life Years (DALYs) from Coronary Heart Disease (CHD) in India. In the last 60 years, CHD prevalence has increased from 1% to 9% in the urban Indian population. For the rural population this increase can be quantified from 1% to 4%. On scrutiny of Report on Medical Certification of Causes of Death (MCCD) by the office of the Registrar General of India1, One can clearly observe that out of the eight major cause groups of death for the period from 1990 to 2013, the group
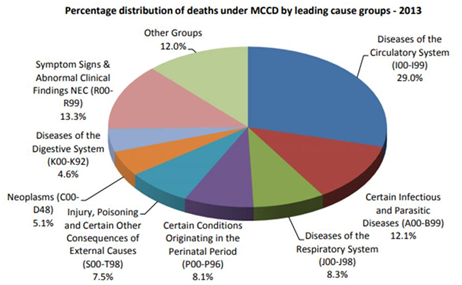
eight major cause groups of death for the period from 1990 to 2013, the group Diseases of the Circulatory system has not only occupied the top most position but its percentage of total deaths has registered an increasing trend.
2. Causes: CVDis a term used to describe different heart or blood vessel problems.It is described as damage atherosclerosis causes to your heart or blood vessels.

Atherosclerosis Is a build-up of fatty plaques in the arteries. Plaque build-up thickens the artery walls and narrows the inside of arteries, which inhibits the blood flow through the arteries to the organs and tissues.Atherosclerosis is the most prevalentreasonbehind the genesis of cardiovascular disease. It can be caused by problems arising out of unhealthy life style, such as an unhealthy diet, sedentary lifestyle, being overweight and smoking.Researchers have always believed that the increase in CHD is driven by industrialisation, urbanisation and related lifestyle changes2. These changes in a society are defined as Epidemiological transitions. Every country undergoes these Epidemiological transitions and this transition is divided into five stages. Stage 1 is the age of pestilence and famines, which is highlighted by infectious diseases, malnutrition and high mortality rate but the mortality due to CVD is low. Stage 2 is the age of receding pandemics, where better public health systems result in decreased mortality from communicable diseases but is marked by emergence of CVD with 10% to 35% mortality. Stage 3 is the age of degenerative and human made diseases, which is indicated by mortality from CVD surpassing mortality from communicable diseases. In this stage 35% to 65% of all deaths happen due to CVD. Stage 4 is the age of delayed degenerative diseases, when CVD and diseases such as cancer are predominant causes of death and CVD leads with >40% of deaths. Stage 5 is the age of inactivity and obesity when declining physical activity leads to epidemics of diabetes, hypertension and lipid abnormalities. Here Deaths due to CVD take on alarming proportions. India is a large and hugely diverse country where various parts of populace can be experiencing any of these stages.
3. Risk Factors:The most important risk factors of heart disease and stroke in India are unhealthy diet, sedentary lifestyle, tobacco use and harmful use of alcohol. These risk factors result inhigh blood pressure levels, high levels of blood glucose, raised blood lipids, overweight and obesity. These can be easily evaluated in primary care facilities and indicate as an increased risk CVD.The Risk factor dynamics in India is undergoing a critical change with an increase seen in CVD factors in rural and slum populations while it is decreasing in the urban populace.Smoking and tobacco use continues to increase in rural and less literate populations, while it is declining in better educated urban populations. The labour-saving technologies have lead to an epidemic of sedentariness in rural households too. Dietary habits in rural households have undergone a see change with higher consumption of fats, saturated fats, trans fats, and processed foods. Rural populace is now matching their urban counterparts in hypertension prevalence in India.There is an increasing abdominal obesity and other cardiometabolic risk factors are also on the rise among the rural populations in India
4. Solution: CVD has taken epidemical proportions in our country and a combination of various interventions are required to address the problem
(a) Primeval Interventions: Aim is to prevent the risk factors by optimising lifestyles and behaviours associated with optimal levels of blood pressure, blood glucose and bodyweight. Encouragement of a tobacco free society will be a big boost to the efforts. Higher tobacco taxes, advertisement bans, taxation of sugar-sweetened beverages and smoke-free policies must be resorted to4. We all must contribute to these efforts by avoiding use of tobacco, trans fats, sugar sweetened beverages and regulate dietary salt intakes.
(b) Primal interventions: Treatment of risk factors has to be ensured across the populace. The treatment of hypertension in India is alarmingly low. Among those diagnosed with hypertension, only 24.9% in rural India and 37.6% in urban India receive any kind of treatment5. Even treatment of diabetes in India is sub optimal with only one third of the patients able to control the glucose levels. A 2016 microsimulation model–based analysis showed that a benefit-based tailored treatment strategy emphasizing lowering of CVD risk was more effective6. The benefit-based tailored treatment strategy could help achieve more than one-third of the WHO’s CVD mortality target. We all can contribute to this intervention by ensuring that the risk factors if diagnosed are taken care of by Medical Practitioners.
(c) Secondary interventions: The use of therapies to prevent recurrence of CVD in India is suboptimal. Cardiac rehabilitation is an important component of a secondary intervention regimen, leading to decrease in overall mortality, CV mortality, and cases of Rehospitalisation. Despite these favourable effects, referral to cardiac rehabilitation is low, even in developed countries, and cardiac rehabilitation is nearly absent in India. We must turn to traditional practices such as Yoga for Cardiac Rehabilitation.
5. Conclusion: CVD is emerging as one of the biggest causes of mortality in India. It also results in massive economic burden on the country. Though Government needs to intervene immediately with Primeval, Primal and Secondary interventions, We as individuals also need to contribute to arrest this pandemic. Taking care of our own health will contribute towards the health of our nation.
References
1.https://censusindia.gov.in/2011/Documents/mccd_Report1/Mccd_2013.pdf
2.T.A. Gaziano, J.M. GazianoEpidemiology of cardiovascular disease Harrison's Principles of Internal Medicine (19th ed.), McGraw Hill, New York, NY (2016), pp. 266.e1-266.e5
3.V. Fuster, B.B. KellyBoard for Global Health. Promoting Cardiovascular Health in Developing World: A Critical Challenge to Achieve Global Health Institutes of Medicine, Washington, DC (2010)
4.Prabhakaran D., Anand S., Watkins D., et al., Disease Control Priorities-3 Cardiovascular, Respiratory, and Related Disorders Author Group (2018) Cardiovascular, respiratory, and related disorders: key messages from Disease Control Priorities, 3rd edition.
5.Roy A., Praveen P.A., Amarchand R., et al.(2017) Changes in hypertension prevalence, awareness, treatment and control rates over 20 years in National Capital Region of India: results from a repeat cross-sectional study.
6. Basu S., Yudkin J.S., Sussman J.B., Millett C. ,Hayward R.A.(2016)Alternative strategies to achieve cardiovascular mortality goals in China and India: a microsimulation of target-versus risk-based blood pressure treatment.